By Tamal Gope, Co-founder & CEO, YORO Health · Reading time: 7 minutes · Bookmark this if you have parents over 65.
A few months ago, one of our patients at the Amanora Township pilot — I’ll call him Patient D, because that’s how he appears in our records — was 89 years old, had survived two coronary bypass surgeries, and was living alone with his daughter checking in twice a week. On the day my nurse first walked into his apartment, his blood pressure read 180 over 90. That is not a number you ignore. That is a number that, in the absence of someone standing in the room with a cuff and a notebook, ends in an ambulance.
What happened next is what I want to write about. Not because it’s dramatic — it isn’t. But because it sits at the heart of a much larger problem in Indian elder care that almost nobody is talking about clearly: the fall, the stroke, the hospital admission — these are the visible events. The decline that precedes them is invisible. Unless someone is measuring.
I’ve spent the past year building a senior care company called YORO Health, with my co-founders Sahil and Deepak, embedding full-time nurses inside Pune’s Amanora Park Town. I am not a doctor. I am a former operator from Cars24, Uber, and Amazon who got pulled into eldercare by the same realization that pulls most people: a parent, a sibling, a number that didn’t sound right. What I’ve learned in the months since is that the gap between what Indian families know about elder health and what is actually knowable is one of the most consequential gaps in this country — and falls are the cleanest place to see it.
How big is this problem actually?
The most-cited numbers in global health are the World Health Organization figures: roughly 28–35% of people over 65 fall every year, rising to 32–42% for those over 70. They are also, unhelpfully for an Indian audience, mostly derived from Western populations.
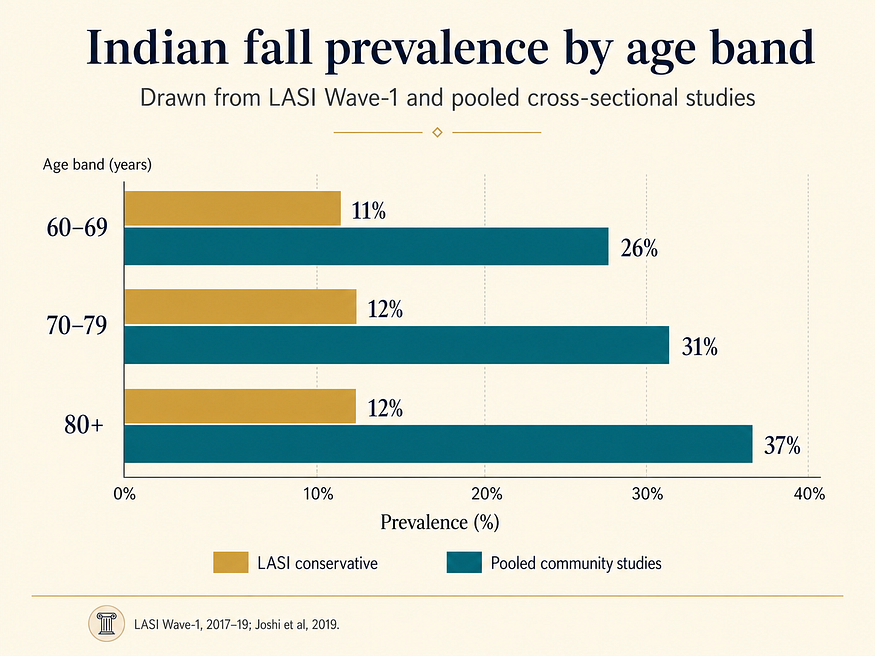
The Indian picture is harder to pin down because we have fewer longitudinal studies, but the evidence is now substantial. A 2019 systematic review in the Journal of Mid-Life Health examined community studies across India and found fall prevalence ranging from 26% to 37% across regions. A 2023 systematic review and meta-analysis pooled the data more rigorously and arrived at approximately 31%. The injury rate that follows a fall is more alarming than the fall itself: 65.6% of Indian seniors who fall sustain some form of injury — fractures in 12.5%, dislocations or sprains in 14.3%, and direct hospital admissions in nearly 20%.
The Longitudinal Ageing Study in India (LASI), the largest dataset of its kind in the country, conservatively places self-reported prevalence at 11–12.5% — almost certainly an undercount, since under-reporting of falls is a well-documented phenomenon, particularly when adult children are the ones asking the questions.
The number that should stop every adult child reading this: roughly one in three Indian seniors over 60 will fall this year. Two in three of them will be injured.
What Patient D’s chart told us, and what it didn’t
Back to Patient D. When my nurse recorded that 180/90 reading, the standard agency response would have been to note it, advise the family to see a doctor, and move on to the next visit. That is what most home-care providers in India do today. It is also why most home-care providers in India do not, in any meaningful sense, change outcomes — they document them.
What we did instead was escalate. The supervisor reviewed the reading within the hour. The family physician was consulted by the daughter the same day. A medication was adjusted. The next visit recorded 152 systolic. The visit after that, 130. The one after that, 150 — a Day-4 rebound that, in isolation, would have looked alarming, but in the context of a continuous record was clearly noise, not signal. By visit five, he was at 125.
This is not an ambulance story. There was no emergency. There was no dramatic save. But somewhere in the counterfactual version of this story, Patient D had a stroke at 88. The pattern that prevented it was visible only because someone was inside the building, capturing the reading, and trusting the previous five readings enough to know what mattered.
Falls work the same way. The visible event — the hip fracture, the head injury, the loss of independence — is preceded by a quiet, measurable decline. A walking pace that has slowed. A grip that doesn’t open a jar anymore. A blood pressure that drops 20 points when standing. None of these things, individually, will make a parent call their child. All of them, together, are the forecast.
The Indian healthcare system has not built the home-based infrastructure to capture this. So most adult children have, in effect, been navigating in the dark — with the only data available to them being the result of the event they were trying to prevent.
The single best predictor of a future fall (and how to measure it at home)
If the medical literature on falls has one consistent finding, it is this: the strongest predictor of a future fall is a previous fall. A senior who has fallen once in the past year has roughly double the risk of falling again.
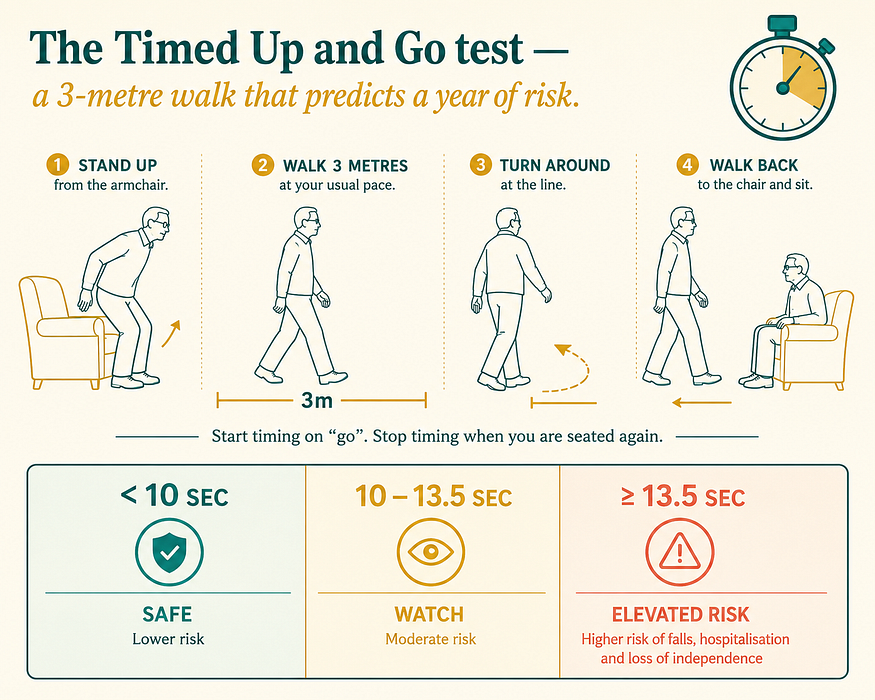
The second-strongest predictor, validated across decades of geriatric research, is performance on the Timed Up and Go test — the TUG Test. It is one of the simplest, most reliable tools in all of geriatrics, and you can administer it at home with no equipment beyond a chair and a stopwatch.
How to do it:
- Have your parent sit in a standard armchair (seat height roughly 46 cm).
- Mark a point 3 metres in front of the chair with a piece of tape.
- On the cue “go,” they stand, walk at their normal pace to the line, turn, walk back, and sit.
- Time the entire action with a stopwatch — start when you say “go,” stop the moment they’re seated again.
The interpretation is well-established in the American Geriatrics Society fall-prevention guidelines. Under 10 seconds is broadly normal. 10 to 13.5 seconds suggests mild decline worth monitoring. At 13.5 seconds or longer, the senior is at meaningfully elevated risk of falling, and a clinical referral to a geriatrician or physiotherapist is warranted.
This is not a substitute for clinical assessment. It is a screening tool — the first thing a primary care physician would do, that you can now do yourself, every three months, sitting in your parent’s living room. Track it over time. The absolute number matters less than the trend.
The risk factors that compound, and what to do about each
A fall is rarely a single cause. The BMC Public Health analysis of LASI data identified the most consistently associated risk factors among Indian seniors. They cluster into four categories, and each has a concrete intervention that does not require expensive equipment.
Vision. Untreated cataracts and uncorrected refractive errors are among the most under-addressed fall risks in India. An annual ophthalmology check is the single highest-yield medical intervention. Bifocals are particularly problematic on stairs; many geriatricians recommend dedicated reading glasses kept separately.
Medications. Polypharmacy — five or more concurrent medications — is associated with significantly elevated fall risk, especially when those medications include benzodiazepines, certain antihypertensives, or sleep aids. A medication review every six months, asking the explicit question “which of these can we deprescribe or reduce?”, is one of the most under-utilized interventions in Indian elder care.
Grip strength and lower-body muscle mass. Sarcopenia accelerates after 70. Grip strength is increasingly used as a bedside proxy for systemic muscle health and is one of the simplest things to track. Resistance training, even with light weights or bands, reduces fall incidence by 25–40% across multiple trials. It does not require a gym. It requires 15 minutes a day.
Postural hypotension. A drop in blood pressure when standing up — common in seniors on multiple medications — causes lightheadedness and is implicated in a meaningful fraction of falls that occur shortly after rising from bed. A home blood pressure check, taken sitting and then again one minute after standing, identifies it in seconds.
In our pilot we track grip strength on every visit. The reason is simple: it changes faster than weight, faster than mobility scores, and it changes before the fall.
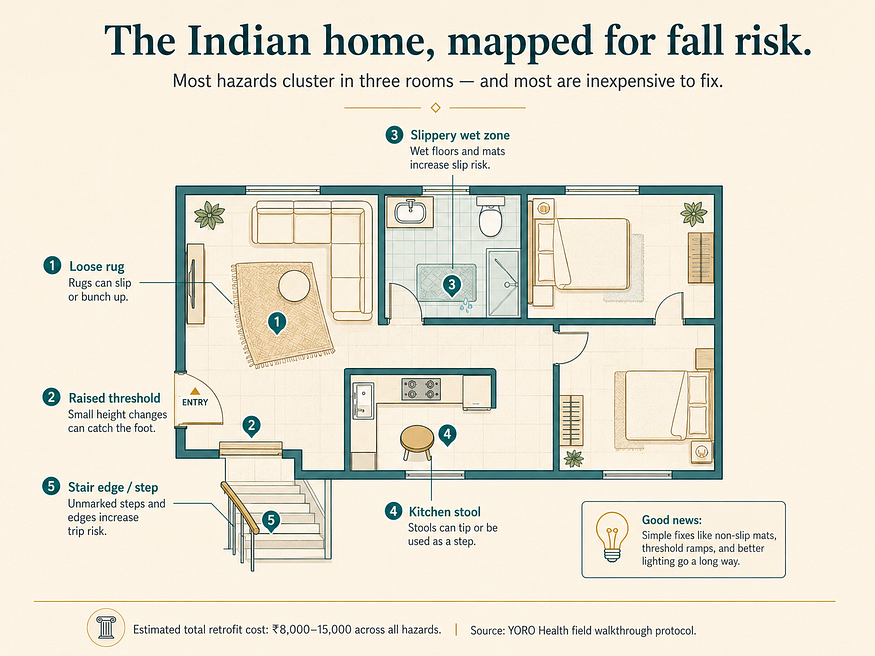
A 12-point home safety walkthrough
If you do nothing else after reading this, do this walkthrough the next time you visit your parents.
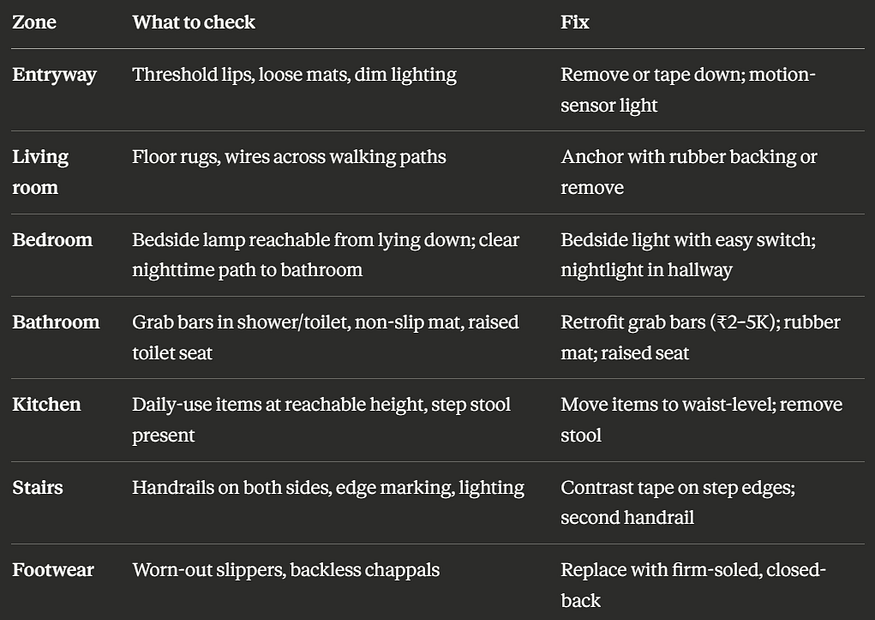
It covers roughly 80% of the modifiable environmental risk factors documented in the Indian fall-prevention literature.
What I’ve actually learned
A year in, the thing I keep coming back to is this: India does not have a knowledge problem in elder care. The risk factors for falls are well-characterized. The interventions are well-validated. Most are inexpensive. What we have is a measurement problem — a missing layer of infrastructure between the senior at home and the clinical system that exists to help them.
Patient D’s blood pressure didn’t drop from 180 to 125 because of a medical breakthrough. It dropped because somebody was in the room, five times in a week, with a cuff and a notebook and a supervisor on the other end of a WhatsApp escalation. That isn’t a technology story. It’s a logistics one. And it’s the one piece of the puzzle that hospitals can’t ship to your parent’s door in 90 minutes, that nursing agencies can’t guarantee, that family caregivers can’t be expected to provide on top of careers and children of their own.
The next fall in your parent’s life is not random. It is being forecast right now, in their grip strength, in their standing blood pressure, in the three seconds their TUG test has slowed since the last time you visited. You do not need a doctor in the house to capture any of this. You need to start measuring.
If we get the measurement part right, India can age in place — at home, near family, with dignity. If we get it wrong, we will continue to lose a generation of elders to events that were entirely visible weeks before they happened.
That’s what I’ve spent the last year building toward. It’s the only honest answer I can offer to the question my mother asked me a year ago, which is the question every adult child in this country eventually asks: who’s actually going to be there when something happens?
The answer, at scale, has to be: someone who was already there. Who was already measuring. Who already knew.
If you’d like a printable copy of the home safety walkthrough, or want to learn more about structured at-home health monitoring for elderly parents, visit yorohealth.com. The next piece in this series — on grip strength as the most under-appreciated vital sign in Indian eldercare — is on our Medium publication.
Further reading
- WHO Falls Fact Sheet
- LASI India Report (Wave-1)
- BMC Public Health: Fall-related injury in Indian older adults
- Systematic review: Health consequences of falls in Indian seniors
- The Timed Up and Go test — original validation
- American Geriatrics Society fall prevention guidelines
About YORO Health — YORO Health embeds full-time nurses inside residential communities to deliver on-demand, structured elder care with sub-10-minute response times and 15-marker health tracking on every visit. Founded in Pune; expanding across India. Learn more at yorohealth.com.