By Tamal Gope, Co-founder & CEO, YORO Health · Reading time: 7 minutes
A few weeks ago, one of my nurses at our Amanora pilot in Pune was sitting with an 89-year-old patient — two coronary bypasses behind him, living mostly alone, daughter checking in twice a week. His blood pressure that morning read 180 over 90. That is not a number you ignore. Five visits later, after a supervisor escalation and a medication adjustment by his family physician, the same patient was at 125 systolic.
This is not a dramatic story. There was no ambulance, no emergency room, no near-miss with mortality. It is, instead, a quiet story about what becomes possible when there is someone physically inside the building, capturing the right reading at the right time, with a chain of escalation behind them that actually works.
I’ve spent the past year building YORO Health with my co-founders Sahil and Deepak, embedding full-time nurses inside residential communities in Pune. We are 12 days into our first formal pilot at Amanora Park Town: 37 completed visits, a 4.8-minute median dispatch time, 33% subscription conversion, clinical patterns flagged in 5 of 13 patients. It is a small footprint. It is also more longitudinal data than most home care providers in this country have collectively captured.
What I want to write about today is not YORO. It is what I have come to understand, after a year inside this work, about the scale of the gap we are all walking toward — and how little of India’s institutional response suggests anyone in policy, in capital, or in healthcare has registered what is actually about to happen.
The trajectory, soberly
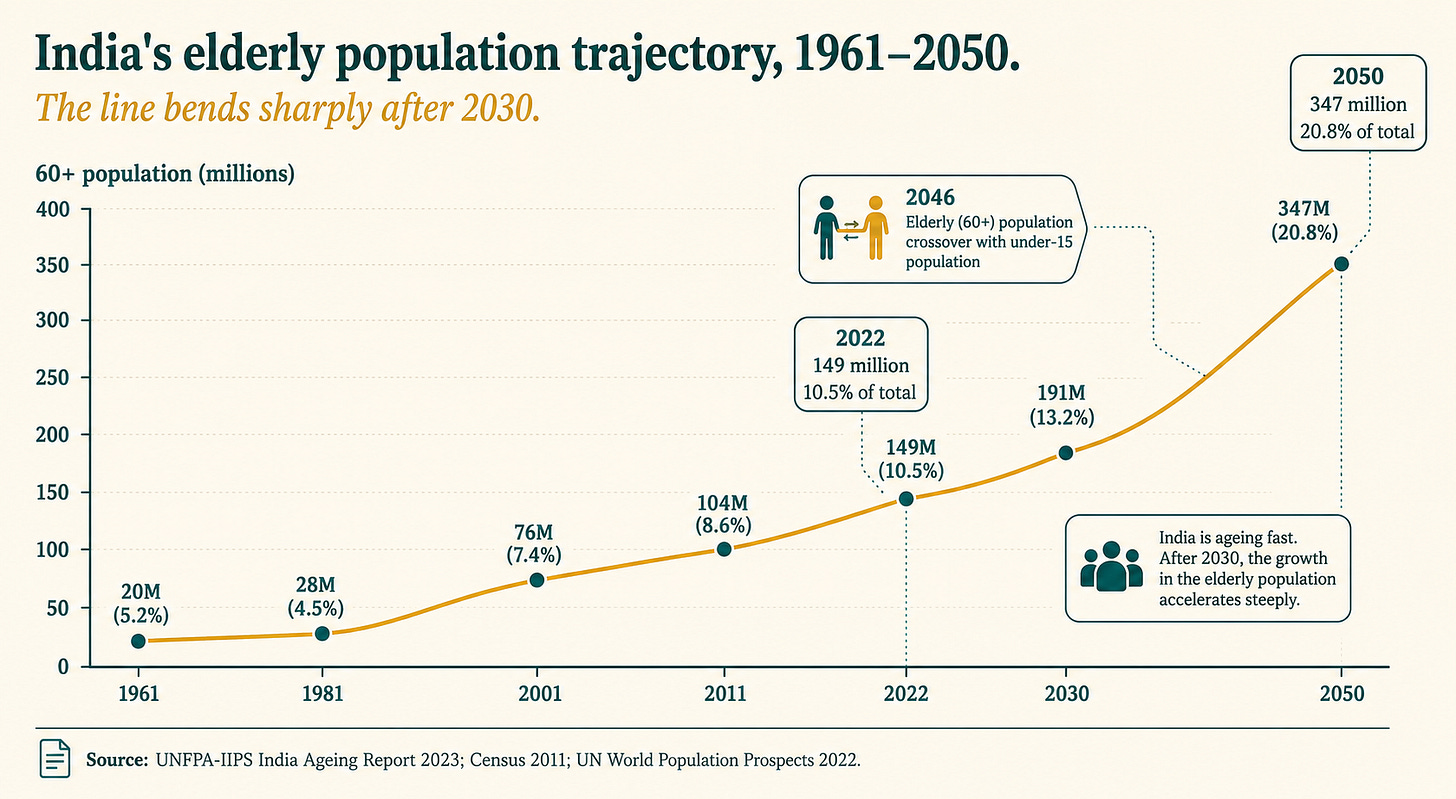
In 2022, India had 149 million people aged 60 and above — 10.5% of the population. By 2050, that number will reach 347 million. A 134% expansion in the elderly cohort, against an overall population growth of just 18%. By 2046, India will have more elderly than children. The country will be older than the United States is today.
This is not a forecast you can argue with. It is a United Nations Population Fund projection built on census data, the Longitudinal Ageing Study in India, and Government of India population projections through 2036. The trajectory is locked.
What is striking, when I started spending real time with this data, is how little of the country’s policy, capital, and institutional design appears to be responding to it. India is currently building roads, airports, semiconductor fabs, and data centres at unprecedented scale. The infrastructure deficit nobody is talking about — the one that will matter most to the largest number of Indian families over the next two decades — is care.
The numbers that should stop you
A few comparisons made this real for me.
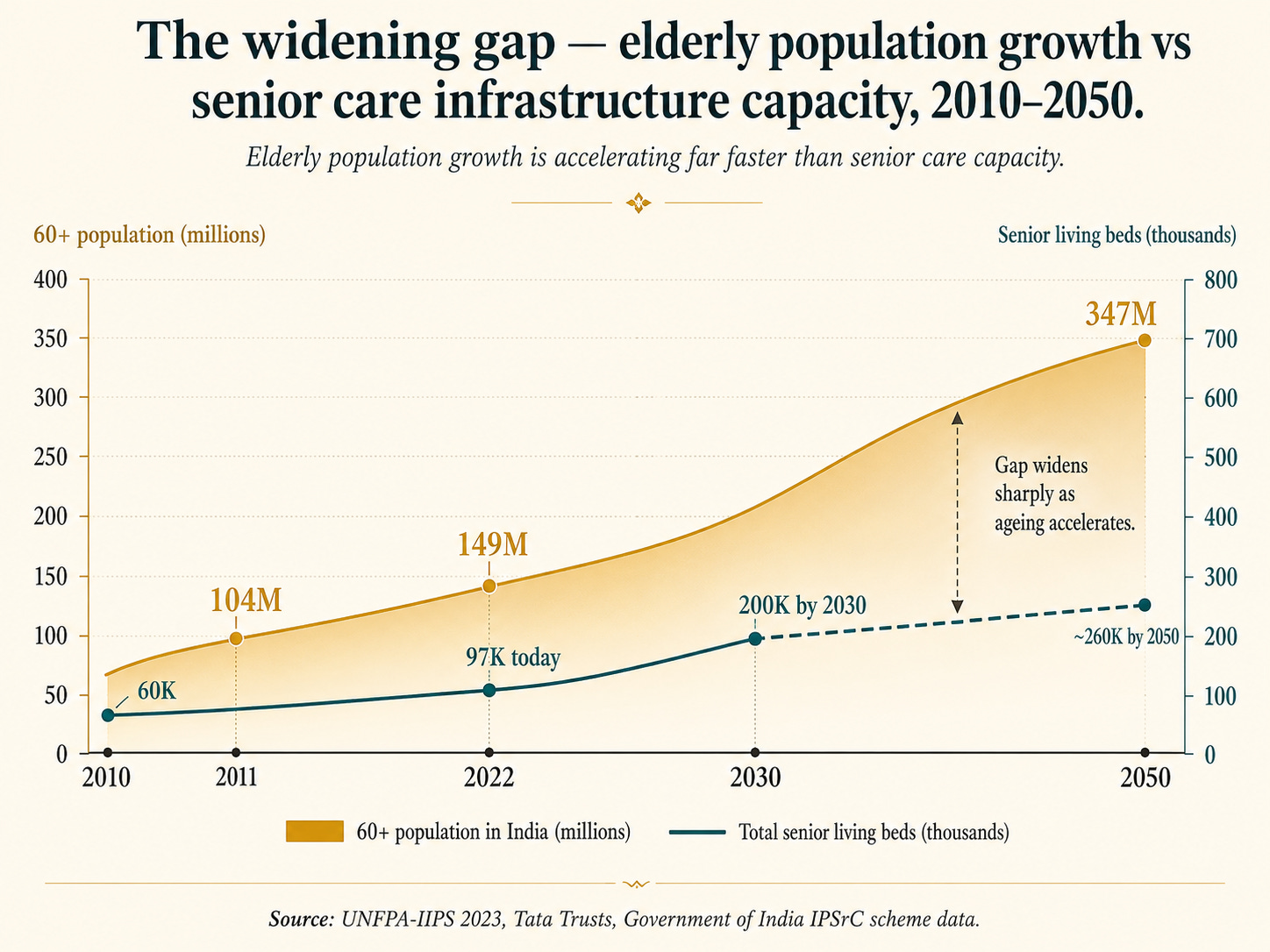
Senior living capacity. A Tata Trusts study estimated India’s total senior living capacity — across luxury communities, mid-market homes, and free or subsidized facilities — at approximately 97,000 beds. Against 149 million elderly, that is 0.65 beds per 1,000 elderly. The United States has roughly 40 beds per 1,000. The OECD average sits between 30 and 50. India is 60 times short of the OECD baseline, and the gap is widening every year, not closing.
Geriatric specialists. India has approximately 1.3 million registered allopathic doctors. Fewer than a handful per million elderly Indians are trained specifically in geriatric medicine. The discipline barely exists as a recognized specialty.
Nurses. India has 3.3 million registered nurses, but very few are trained in geriatric care, and most are deployed in hospitals, not in community or home settings. The senior at home is one of the most underserved patients in the entire Indian healthcare system.
Government schemes. India’s flagship elder welfare program, the Integrated Program for Senior Citizens, maintains 1,658 old age homes with a total annual disbursement of ₹321 crores. Divided across 149 million elderly, that is roughly ₹21 per elderly Indian per year. By any conceivable benchmark, this is not a senior care policy. It is a rounding error.
Insurance. Urban senior health insurance penetration is approximately 38%. Rural penetration is dramatically lower. Most Indian seniors who need care pay for it out of pocket, often at the moment when the family’s savings are already stretched thin by mortgages and education expenses.
The Indian elderly population is not just growing. It is growing in a country whose health, housing, and welfare systems were calibrated for a population that was supposed to remain young.
Why this gap exists, structurally
The most reasonable assumption is that India’s deficit in elder care infrastructure is a function of the country still being relatively poor. The longer I’ve sat with this, the less I believe that’s the right explanation.
India’s demographic transition is unusually fast. Most countries that aged at this scale — Japan, France, Western Europe — did so over a century or more. India is compressing the same shift into roughly four decades. The LASI Wave-1 report shows the 60+ population grew by 103% between 2000 and 2022, and the 80+ cohort grew by 128% in the same period. Speed is the enemy of infrastructure. Roads can be built in five years. Geriatric residencies, RWA-embedded care models, and assisted living developments take ten to fifteen.
The family caregiver model is breaking, quietly. Indian elder care has rested almost entirely on intergenerational households — the working-age daughter-in-law, the unmarried daughter, the joint family. That model is dissolving on multiple axes simultaneously. India’s total fertility rate is now 1.9 — below replacement. Urban migration has separated working-age children from elderly parents by thousands of kilometres. Female workforce participation, which is rising in urban India, removes the historically default unpaid caregiver from the household. None of this is reversible. All of it is happening before any institutional replacement has been built.
The diaspora is a complicating accelerant. India’s 35.4 million-strong diaspora — the largest in the world — sends home $136 billion in annual remittances. But money cannot solve the proximity problem. An adult child in San Jose or Singapore can fund care for a parent in Pune; they cannot, by the laws of physics, be the care. The diaspora’s relationship with ageing parents in India is the single largest under-served customer segment in Indian healthcare.
Capital has been slow to recognize the category. A Blume Ventures analysis identified only 13 venture-funded eldercare startups in India as of 2024 — against thousands in adjacent categories like fintech and food delivery. The Indian senior care market is projected to reach $11 billion by 2030, but funding has lagged market formation by years. Most existing providers are family-run nursing agencies operating on margins too thin to invest in clinical protocols, technology, or longitudinal data infrastructure.
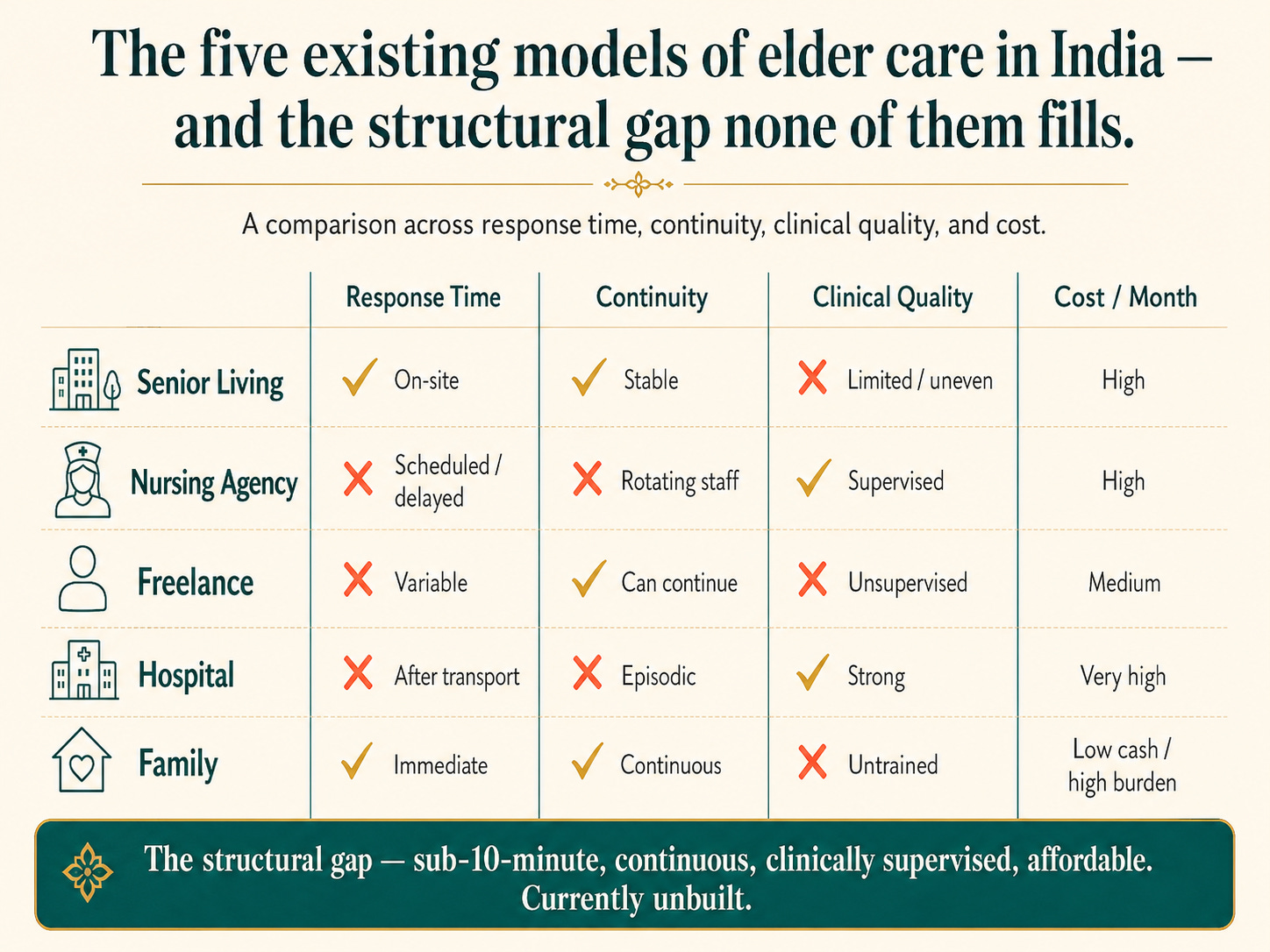
The five options a family has today, and why none of them works
When a family I speak to needs care for an ageing parent, they have five options. I’ve watched every one of them fail in different ways.
Premium senior living communities at ₹70,000 to ₹1.5 lakh per month. Excellent for the small segment that can afford it. Out of reach for less than 1% of Indian seniors.
Nursing agencies like Portea, Care24, and Apollo Homecare. ₹15,000 to ₹50,000 per month, hub-and-spoke dispatch with response times of 45 to 90 minutes, a different nurse on every visit, quality control that varies dramatically, no structured health data capture.
Freelance attendants. ₹12,000 to ₹22,000 per month, unverified credentials, no SLA, no clinical oversight. The default option for most middle-class families. The risk profile is well-documented and largely uninsured.
Hospital home health programs. Excellent clinical depth in the metros, but dispatch times approaching 90 minutes and prices that rival senior living.
Family-managed care. Free in cash terms, expensive in opportunity cost. Increasingly unsustainable as families distribute geographically.
None of these scales. None dispatches a trained nurse to a parent’s door in under 10 minutes. None captures the kind of longitudinal health data that would let a family doctor actually see the trajectory of a senior’s health rather than reacting to events. The 89-year-old at Amanora I opened this essay with would have, under any of the five existing models, been a hospital admission waiting to happen.
What a working response would look like
The infrastructure India needs over the next two decades is not, in the main, more old age homes. It is a distributed, residential-cluster-embedded layer of trained caregivers — supported by structured health data capture, clinical supervision, and an escalation chain back into the formal hospital system when something requires it.
This is, broadly, the model that has worked in markets that have already aged. Honor in the United States, valued at $1.25 billion, runs a network of more than 100,000 full-time employed caregivers delivering scheduled and on-demand visits with 99.9% shift fulfillment. Japan’s Long-Term Care Insurance system has built population-scale infrastructure for in-home senior support since 2000. Scandinavia has run municipal home-help schemes for decades.
The Indian version will look different — denser residential clusters, more reliance on WhatsApp and Aadhaar-linked digital records, more sensitivity to the diaspora customer, almost certainly more public-private partnership — but the architecture is the same. Trained caregivers, embedded close, supported by structured data, integrated with clinical care. None of this is technologically exotic. It is, however, operationally exacting. And it has to be built starting now.
The capital required is not trivial. The labour force is available — 3.3 million registered nurses and over 5,000 nursing institutions training 300,000+ graduates a year. The regulatory framework, through the Ayushman Bharat Digital Mission and the DPDP Act 2023, is finally in place. What is missing is the build.
Why I think this matters more than almost anything else right now
I came to elder care from operating roles at Cars24, Uber, and Amazon. I am not a clinician. I came to this work because of a question my family was asking — the same question every adult Indian child eventually asks — who is actually going to be there when something happens?
What I have learned, building YORO, is that the answer at scale cannot be a hospital 90 minutes away. It cannot be a freelance attendant whose credentials nobody verified. It cannot be a senior living facility most Indians cannot afford. It cannot be a daughter on a flight from California.
The answer has to be: someone who was already there. Someone who was already measuring. Someone who already knew.
That is a very large infrastructure project. It is going to require capital, policy attention, hospital partnerships, and a generation of operators who decide to build it. None of these will arrive on their own.
If you are an investor reading this, the silver economy is one of the most under-allocated thematic in Indian capital markets. If you are a policymaker, the National Program for Health Care of the Elderly needs a budget with at least one more zero. If you are a hospital administrator, your readmission rates are being driven by the absence of the layer beneath you. If you are an adult child of ageing parents — the largest constituency, and the one that ultimately matters most — start the conversation now, while everyone is healthy enough to plan.
India is going to age. It is going to age fast. The question is whether the infrastructure to support that ageing gets built in time — or whether a generation of Indian families will be left navigating it without help.
I know which version I’m working on. I hope a lot more of us choose the same.
Further reading
- UNFPA India Ageing Report 2023
- Longitudinal Ageing Study in India (LASI)
- Tata Trusts — Report on Old Age Facilities in India
- WHO India — Ageing and Health
- Blume Ventures — Indian Eldercare Blueprint
- Ayushman Bharat Digital Mission
About YORO Health — YORO Health embeds full-time nurses inside residential communities to deliver on-demand, structured elder care with sub-10-minute response times and 15-marker health tracking on every visit. Founded in Pune; expanding across India. Learn more at yorohealth.com.